
Translate this page into:
Ultra-low-frequency-transcutaneous electric nerve stimulation for recording cameo surface and detachable cheek plumpers for enhanced complete denture esthetics
*Corresponding author: Ambika K. Narayanan, Division of Prosthodontics and Crown and Bridge, Department of Dental Surgery and Oral Health Sciences, Armed Forces Medical College, Pune, Maharashtra, India. drambika7n@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Gowda EM, Narayanan AK, Kumar RV. Ultra-low-frequency-transcutaneous electric nerve stimulation for recording cameo surface and detachable cheek plumpers for enhanced complete denture esthetics. Asian J Oral Health Allied Sci 2021;11:1.
Abstract
Severely resorbed completely edentulous maxillary and mandibular arches from long-term complete edentulism may pose a treatment challenge for the treating prosthodontist. The loss of teeth, over a period of time, can lead to gross facial disfigurement and also has great psychological effect. The loss of teeth also has effect on the musculature and supporting tissues which may lead to muscle wasting and dystrophy. Ever since its introduction in 1971, Transcutaneous Electrical Nerve Stimulation (TENS) has been used in dentistry for various treatment modalities and it is especially indicated in management of tempo-mandibular dysfunctions (TMDs). TENS being a non-invasive, non-technique sensitive, and easy to use technique has evolved rapidly over the years as an adjunct in management of various dental therapies. Two case reports of completely edentulous patients are presented here, where ultra-low-frequency-TENS (ULF-TENS) was used as an aid in cameo surface recording and customizing the magnet retained cheek plumper within the physiological and functional limits of the orofacial musculature complex for rehabilitation with complete denture prosthesis.
Keywords
Cameo surface
Cheek plumper
Ultra-low-frequency-transcutaneous electric nerve stimulation

INTRODUCTION
The publication of the “Gate Control Theory” by Melzack and Wall in the year 1965, gave a breakthrough for the development of transcutaneous electrical nerve stimulation (TENS) units. Since 1965, TENS has become known worldwide and is also considered to be one of the most common therapeutic resources used in clinical practice for the relief of chronic and acute pain. However, its use in dentistry was initiated in 1969 when the myomonitor was introduced.[1] The use of TENS into clinical practice in prosthodontics increased in 1971, when Jenkelson suggested it as an alternative to conventional border molding.[2] Various studies in the literature have shown that application of TENS stimulated a change in the biochemical and physiological muscular condition; which lead to muscle relaxation.[3,4] Ultralow-frequency-TENS (ULF-TENS) consists of applying an ultra-low-frequency, pulsed, and rhythmic electrical currents.[5] They are transmitted through four surface electrodes which are applied on the skin surface with potential to stimulate the peripheral nerves to produce various physiological effects.
Excessive resorption of the denture bearing area is clinically challenging in terms of achieving optimal stability and esthetics due to impairment of muscle tone and skin tonicity. This sinking of cheeks leads to increased unesthetic appearance of face.[4] These problems, if not corrected, may lead to unsuccessful complete denture therapy. Several methods have been described in literature for plumping or supporting the buccal flange of dentures to improve the outcome of the complete dentures. Even though numerous techniques have been advocated to record the cameo surface and use of cheek plumpers to enhance the esthetics and support of complete denture, accurate recording the cameo surface and making of cheek plumpers within the functional and physiological limits remains a challenge or technique sensitive. To overcome the constraints of these techniques, ULF-TENS may be used to record the cameo surface and cheek plumpers, which has been highlighted through these case reports.
CASE DESCRIPTION
Case report 1
A 84-years-old man reported to the Department of Prosthodontics & Crown and Bridge with a chief complaint of “loose dentures” since past 4 years. On eliciting the patients’ dental history, the patient reported that he had undergone extraction of all his teeth 14 years back due to periodontal and caries problem. Since then, patient has been using two different sets of complete dentures, but was not satisfied due to improper fit of the dentures and change in facial features [Figure 1a and b].
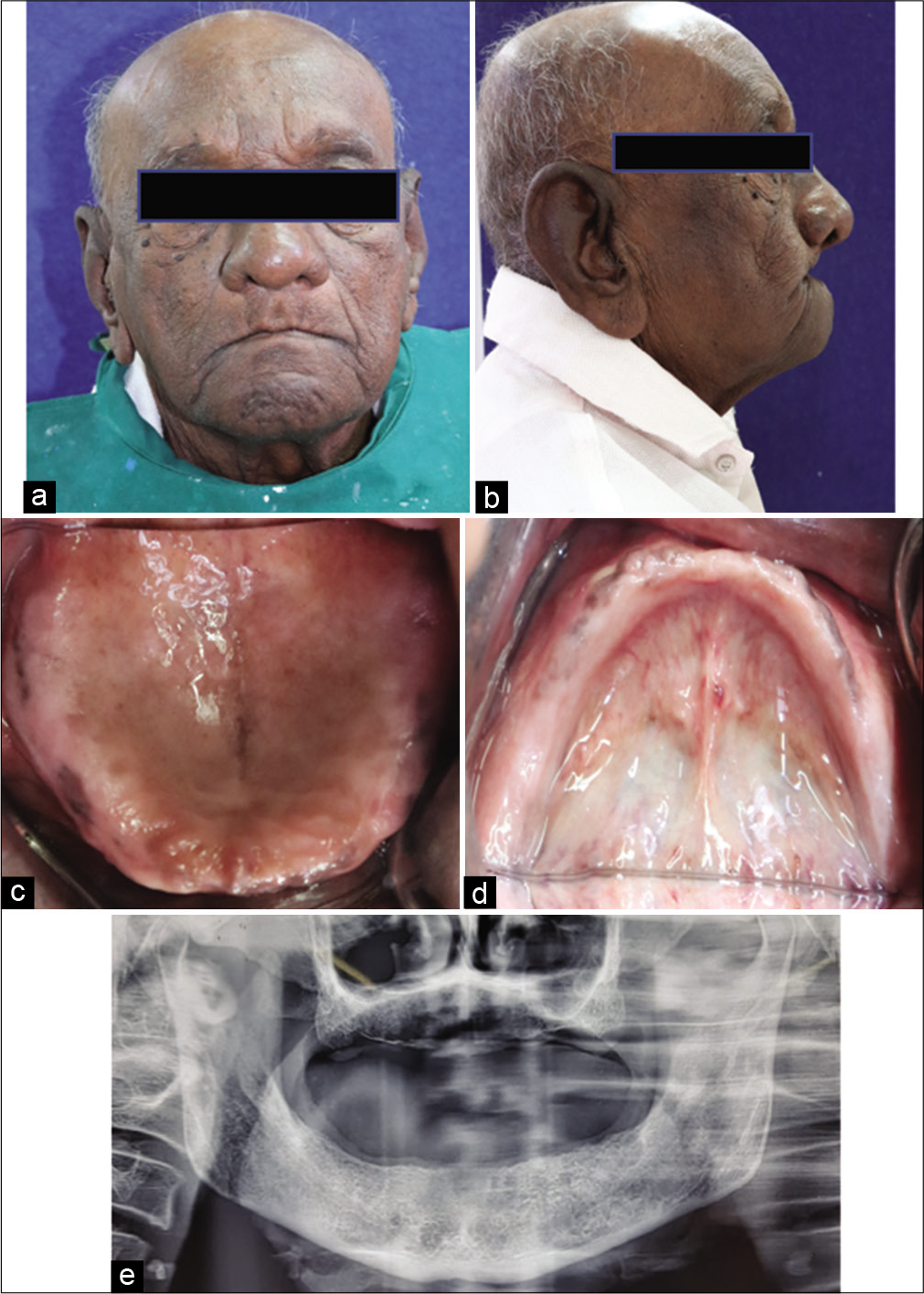
- (a) Pre-operative frontal view, (b) Pre-operative lateral view, (c) Intraoral view (Maxilla), (d) Intraoral view (Mandible), (e) OPG of patient.
During general clinical examination, it was observed that the patient was having difficulty in articulation of words and sentences with slight slurring of speech, which suggested poor neuromuscular coordination. Patient also reported that he was diagnosed with inflammatory myopathy and was on medication since past 8 years under supervision. Based on the clinical examination and radiographic evaluation, the patient was diagnosed as Prosthodontic Diagnostic Index Class I edentulous maxillary and mandibular residual ridges along with inflammatory myopathy [Figure 1c-e]. A treatment plan was formulated to rehabilitate edentulous arches with conventional heat polymerized polymethylmethacrylate resin prosthesis. However, considering the poor neuromuscular coordination of orofacial musculature and inability to follow commands, “ULF-TENS” was used to make the final impression and record the cameo surface of the prosthesis.
ULF-TENS equipment (BLD T250 TCH ULF-TENS Stimulator) containing two electrodes were applied in the posterior triangle of the neck and two were applied in the preauricular region [Figure 2a and b].[3] The ULF-TENS unit was set to operate in continuous mode. The current was gradually increased from 0 to 20 mA, according to patient’s tolerance ensuring control of the left and right sides for the corresponding muscles. Forty minutes of muscle stimulation were given.[4]
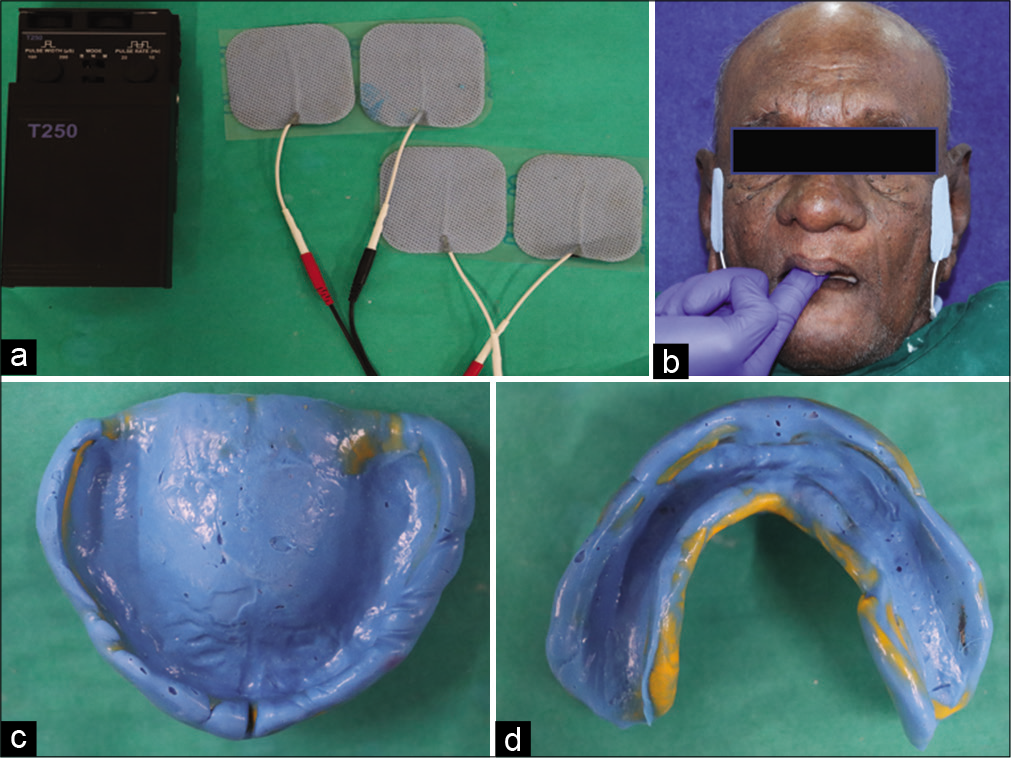
- (a) Ultra-low-frequency-transcutaneous electric nerve stimulation (ULF-TENS) apparatus, (b) ULF-TENS application in situ, (c) Maxillary final impression, (d) Mandibular final impression.
Border molding and final impression was made using polyvinylsiloxane elastomeric impression material with ULF-TENS still in function [Figure 2c and d]. The routine method of using sectional border molding with the operator and patient various functional movements was not followed in this patient. The active stimulation using ULF-TENS, aided in making of a physiologic and functional recording of the border molding and final impression. Jaw relations were recorded and transferred to a semi-adjustable articulator. Teeth were arranged in bilateral balanced occlusion and try in was done.
Tray adhesive was applied over the cameo surface and polyvinylsiloxane elastomeric material (Virtual; Monophase) was applied over the labial and buccal surface of the maxillary denture with the ULF-TENS unit still in function [Figure 3a]. Maxillary denture base was left in position with no functional movements till the material set. The ULF-TENS application led to recording of cameo surface in harmony to functional and physiological movement of orofacial musculature. Similar procedure was performed for mandibular denture [Figure 3b]. Cameo surface on palatal side of maxillary prosthesis and lingual side of mandibular prosthesis was recorded with same material asking the patient to perform various functional movements. The prosthesis was acrylized and processed in conventional manner. The finished prosthesis was delivered to the patient, where a marked improvement in patient’s esthetics was observed with improved comfort reported by the patient [Figure 3c and d].
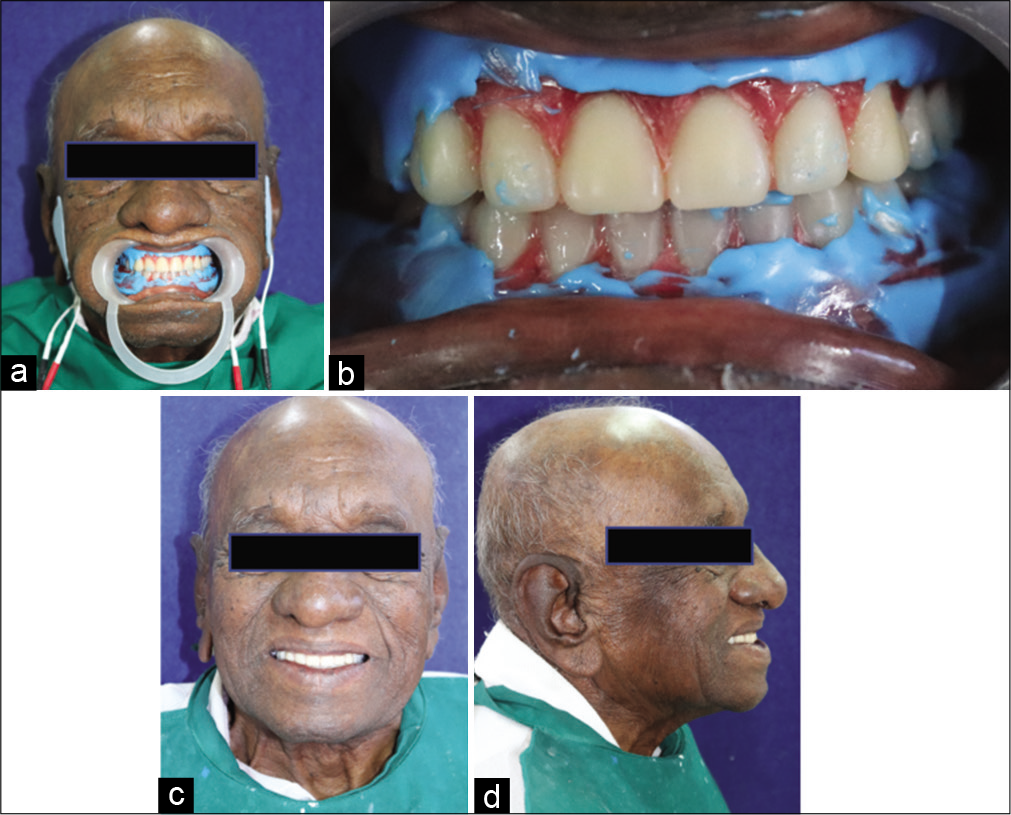
- (a) Ultra-low-frequency-transcutaneous electric nerve stimulation application in situ, (b) Intra-oral view, (c) Post-operative frontal view, (d) Post-operative lateral view.
Case report 2
A 76-year-old male patient, who is farmer by occupation reported to the Department of Prosthodontics & Crown and Bridge with complaint of loss of teeth and unesthetic appearance of face. On eliciting the history, it was revealed that patient had a history of extraction of all his teeth due to teeth mobility 8 years back. Extra-oral examination [Figure 4a and b] revealed a sunken appearance of cheeks, decreased lower facial height, and prognathic appearance. The intra-oral examination revealed severely resorbed maxillary and mandibular edentulous arches [Figure 4c-e]. Various treatment options were discussed with the patient and an implant-supported prosthesis was ruled out because of cost factor. The treatment plan decided was to rehabilitate the patient using removable complete denture prosthesis and plumping of cheeks using cheek plumpers attached to maxillary denture base using magnets.[6] The advantage of this cheek plumper, in addition to being completely detachable, was that it was recorded using ULF-TENS when the oral and peri-oral musculature were in functional and physiological harmony.
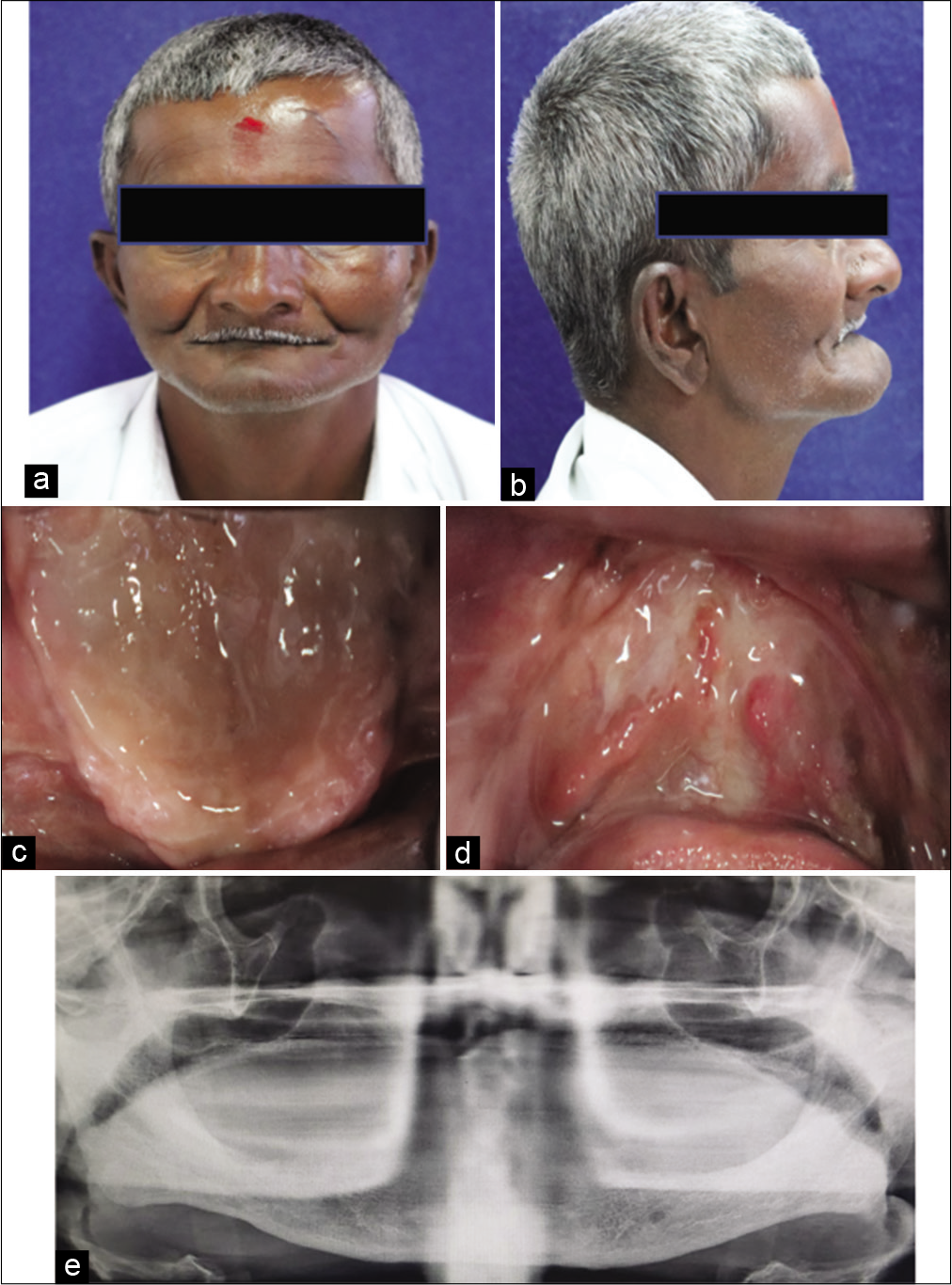
- (a) Pre-operative frontal view, (b) Pre-operative lateral view, (c) Intraoral view (Maxilla), (d) Intraoral view (Mandible), (e) OPG of the patient.
Conventional steps for complete denture fabrication were carried out till try-in of waxed up denture stage. To record the cheek plumpers, ULF-TENS was used. The ULF-TENS equipment was set at the same gradient values as previously mentioned for recording of cameo surface [Figure 5a]. Rectangular strip of putty type polyvinylsiloxane material (Zhermack elite HD + putty soft) was adapted on the maxillary denture and inserted into the patients mouth while the muscles are being stimulated with ULF-TENS [Figure 5b]. The plumpers get molded automatically according to muscular movements (twitching). No functional or manual molding was performed or was needed.
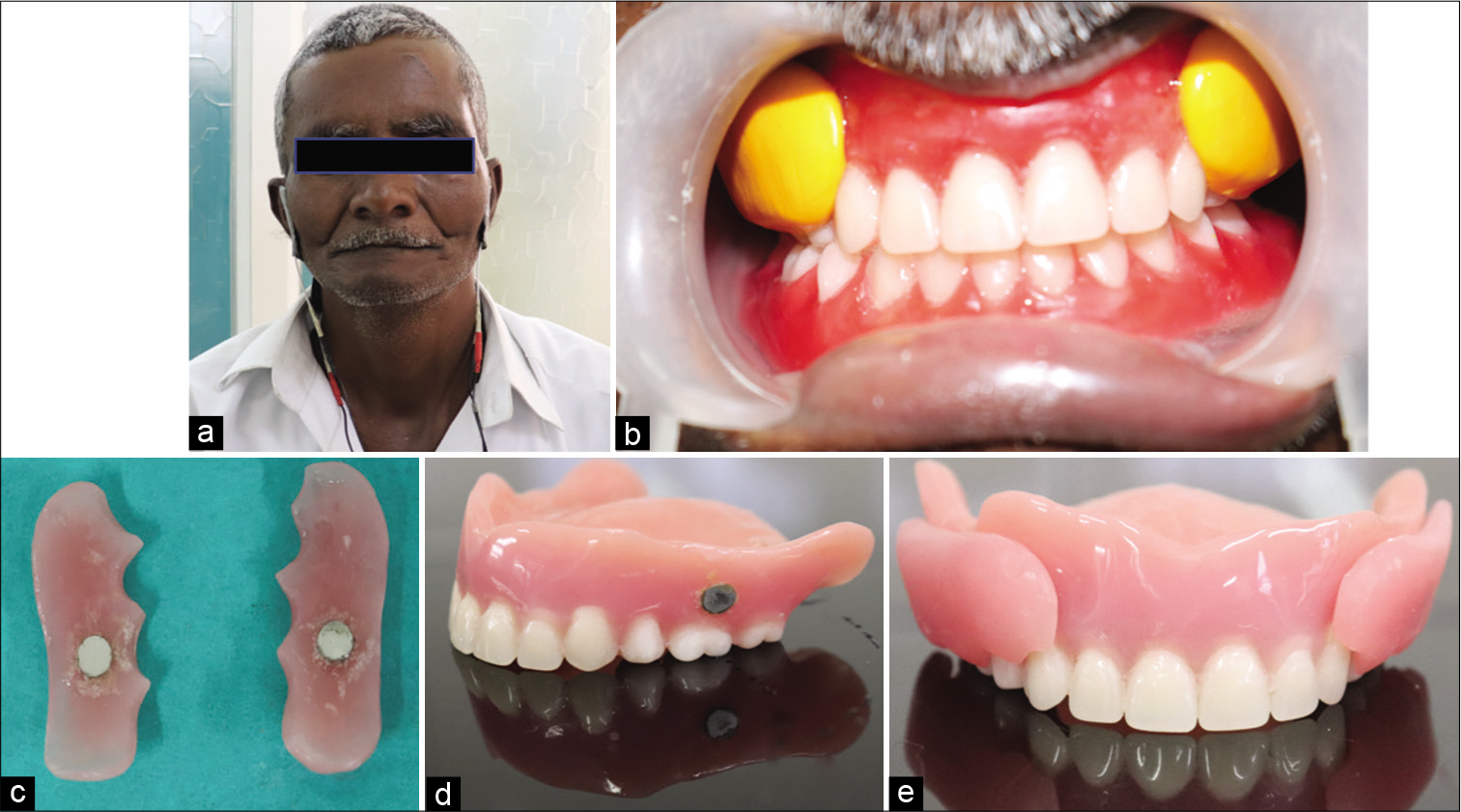
- (a) Ultra-low-frequency-transcutaneous electric nerve stimulation application in situ, (b) Recording cheek plumpers, (c and d) Dyna magnetic attachments on cheek plumper and maxillary denture base, (e) Maxillary denture with attached cheek plumpers.
The cheek plumpers were processed in conventional manner as for any dentures. Dyna magnets were incorporated in the maxillary denture base and the cheek plumpers [Figure 5c-e]. A thin layer of autopolymerizing resin was used to cover the magnets to avoid corrosion. In the extra-oral view, the difference in the depression of the cheeks with and without cheek plumpers and a considerable fullness of cheeks increasing the aesthetic appeal in the patient can be observed [Figures 6a-c].[7] The patient was given instructions regarding usage and maintenance of the prosthesis.
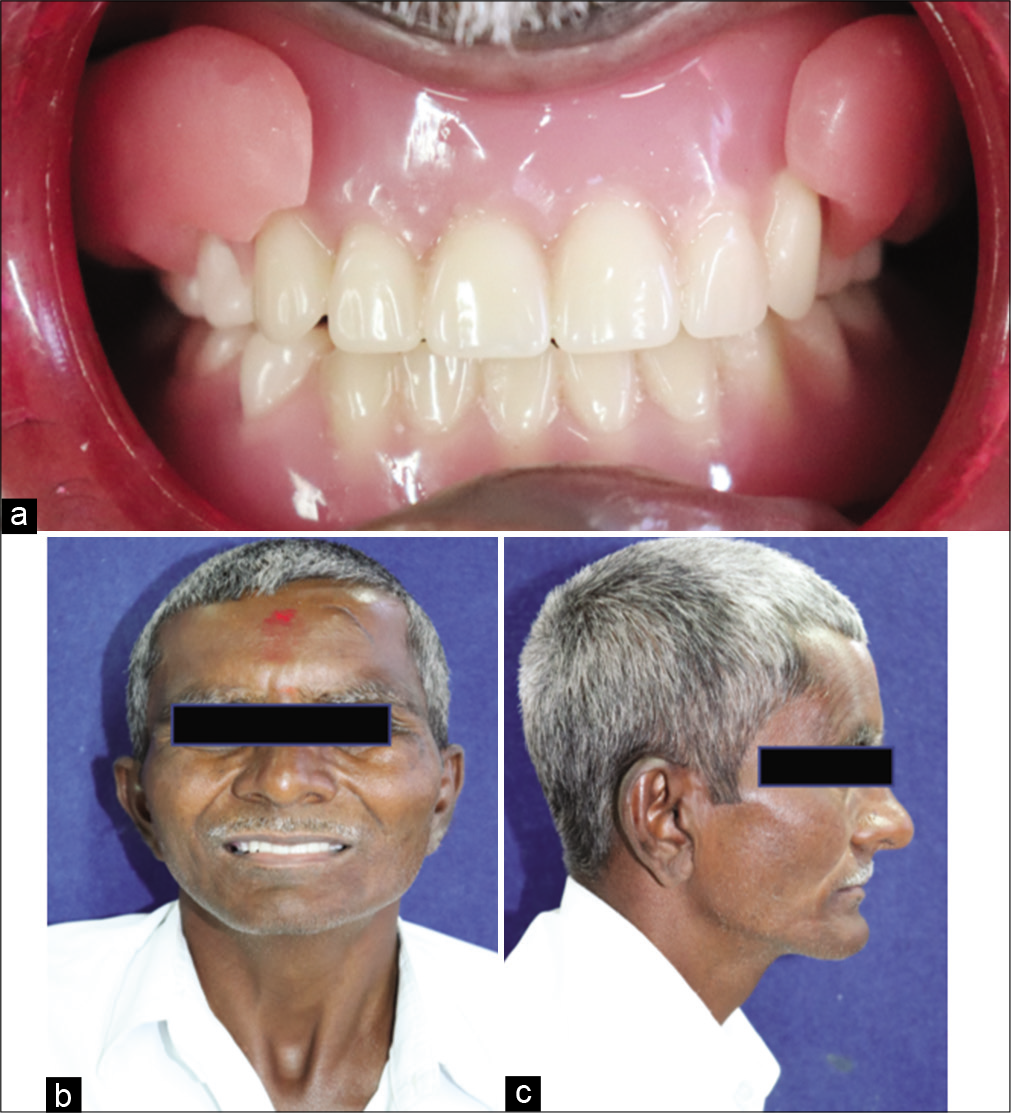
- (a) Prosthesis in situ, (b) Post-operative frontal view, (c) Post-operative lateral view.
DISCUSSION
In the recent years, TENS has gained popularity, as a noninvasive means of management of chronic facial pain, bruxism, and as an adjunct for other dental therapies including prosthodontics. Clinically, application of TENS utilizes two levels of frequencies, that is, low frequency and high frequency. In low frequency TENS, frequency of stimulation is <10 Hz where as in high frequency TENS it is >50 Hz. The term ULF is used when frequency of <4 Hz is used for stimulation.[3]
In medical application, high frequency TENS serves to block stimulus conduction in nerve fibers of nociceptive system. The low-frequency stimulus with a relatively high intensity, affects the motor neurons of the muscles. Several authors have evaluated the effect TENS on electromyographic activity of masticatory muscles in TMD patients. Chipaila et al.[3] and Kamyszek et al.[8] concluded that ULF and low amplitude TENS applied for 60 min in TMD patients are able to relax the masticatory musculature.
Esclassan et al.[9] and Cooper[10] evaluated the effect of ULF-TENS on electromyographic activity of masticatory muscles and reported a decreased electromyographic activity of hyperactive muscles. In the position paper of the International College of Cranio-Mandibular Orthopedics in 2011, Cooper[10] stated that “ULF-TENS is an active therapeutic device that affects relaxation of masticatory and mandibular postural muscles by the use of low frequency, low current stimulation of the mandibular division of the trigeminal nerve, and a branch of the superficial facial nerve. TENS is used during the treatment to achieve a therapeutic neuromuscular balance.[9,10]
To restore facial esthetics, adequate thickness of dentures flanges is required to give support to the facial muscles. Restoring the shrunken cheeks to their natural fullness can be done by adding extra support to the denture flange area. However, increasing the bulk at denture flange area will lead to loss of stability as it will interfere with muscle function (as the flange is not recorded in physiologic position of muscles), loss of retention due to increased weight of the prosthesis.[4,6]
In the first case report, the patient history revealed inflammatory myopathy, application of ULF-TENS helped in recording cameo surface which was compatible with patients’ neuromuscular status. In the second case report, where esthetics was main concern of patient, a detachable magnet retained cheek plumper or cheek lifting appliance was fabricated using ULF-TENS, which offered more advantages in terms of improved esthetics, stability, and support of the prosthesis. To avoid arbitrary bulk adding of material, ULF-TENS was used as a modality to acquire a physiologic state of the muscle activity, in which addition of a moldable polyvinylsiloxane based material was used to record the proper extent of the cheek plumper, which did not hamper the muscle function. Electrodes stimulated the seventh cranial nerve innervating the buccinators, orbicularis oris, and levator labii superioris muscles and the mandibular division of the trigeminal nerve innervating the tensor veli palatini muscle.[3] The ULF-TENS was used as an aid to achieve acceptable esthetics and speech and overall enhances patient satisfaction.[4]
The advantage of the described technique using ULF-TENS instead of the conventional method of recording the extent of cheek plumper is a reduction in inconsistencies associated with manual and functional molding (operator-determined and patient-determined) that may occur if the patient cannot comply or correctly perform functional movements. Furthermore, both the cameo surface and oral and perioral musculature are in harmony without loss of stability of dentures. Thus, the suggested method using ULF-TENS is useful for patients who cannot comply with dental surgeon’s direction or have poor neuromuscular coordination.
However, the use ULF-TENS should be done with precaution. ULF-TENS is generally regarded as safe but it has risks just like any other medical procedure. For instance, if the electrical current is too high or the electrodes are placed on the wrong part of the body, this can burn or irritate the skin. The electrical impulses that a ULF-TENS unit produces may cause a buzzing, tingling, or prickling sensation, which some people may find uncomfortable.[3] It being electrostatic equipment is contraindicated in patients with pace makers, epilepsy, cerebrovascular, and cardiovascular problems and pregnancy.
CONCLUSION
A satisfactory outcome can be attained in patients with poor neuromuscular incoordination and in patients with resorbed ridges by accurately recording a physiological zone of muscle activity that aids in improving denture stability and esthetics. A method of recording cameo surface and cheek plumpers using ULF-TENS that helps in physiological adaptation of the prosthesis to orofacial musculature has been described in these reports.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Neural conduction of the myo-monitor stimulus: A quantitative analysis. J Prosthet Dent. 1975;34:245-53.
- [CrossRef] [Google Scholar]
- The effects of ULF-TENS stimulation on gnathology: The state of the art. Cranio. 2014;32:118-30.
- [CrossRef] [PubMed] [Google Scholar]
- Cameo surface recording in complete denture fabrication using transcutaneous electrical nerve stimulation: A clinical report. J Prosthet Dent. 2017;118:127-30.
- [CrossRef] [PubMed] [Google Scholar]
- Physiological aspects of masticatory muscle stimulation: The myomonitor. Quintessence Int Dent Dig. 1972;3:57-62.
- [Google Scholar]
- Artificial cheek plumper's: A step ahead in denture esthetics-a case report. Indian J Stomatol. 2011;2:134-7.
- [Google Scholar]
- Patients' satisfaction with dental esthetics. J Am Dent Assoc. 2007;138:805-8.
- [CrossRef] [PubMed] [Google Scholar]
- Electromyographic evidence of reduced muscle activity when ULF-TENS is applied to the Vth and VIIth cranial nerves. Cranio. 2001;19:162-8.
- [CrossRef] [PubMed] [Google Scholar]
- Optimal duration of ultra low frequency-transcutaneous electrical nerve stimulation (ULF-TENS) therapy for muscular relaxation in neuromuscular occlusion: A preliminary clinical study. Cranio. 2017;35:175-9.
- [CrossRef] [PubMed] [Google Scholar]
- International College of Cranio-Mandibular Orthopedics (ICCMO)Temporomandibular disorders: A position paper of the international college of cranio-mandibular orthopedics (ICCMO) Cranio. 2011;29:237-44.
- [CrossRef] [PubMed] [Google Scholar]




