
Translate this page into:
Oral health care in children with Down syndrome: Indian parents’ perceptions on its impact, and challenges faced
*Corresponding author: Rhythm Bains, Department of Conservative Dentistry and Endodontics, King George’s Medical University, Lucknow, Uttar Pradesh, India docrhythm77@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Gupta N, Bains R, Gupta A, Ramchandran S, Bains VK. Oral health care in children with Down syndrome: Indian parents’ perceptions on its impact, and challenges faced. Asian J Oral Health Allied Sci. 2025;15:5. doi: 10.25259/AJOHAS_25_2024
Abstract
Objectives
The study explored parents’ perception regarding the impact of Down syndrome on oral health and the challenges faced in availing dental care for their children.
Material and Methods
Interviews were conducted with the parents and oral health care providers (OHCP). A questionnaire was developed and shared as a Google Form amongst participants. The sections of the questionnaire were as follows: Demographics (nine questions), schooling (three questions), general health of the child (four questions), oral health (nine questions), impact on quality of life, and barriers faced (eight questions) and the last section open-ended. The data were analyzed using descriptive analysis and expressed in numbers and percentages.
Results
Although 60% of parents reported their child’s oral health as good, the quality of life was affected by lack of clarity of speech (65.1%), presence of cavities (35.4%), difficulty in chewing (34.9%), distress due to toothache (19.5%), and absence from school (8.2%). About 24% of respondents reported that they had not visited a dentist yet. About 31.3% of parents reported that they are not able to find oral health care facilities catering to special needs, and 19% reported that they had to travel a long distance to see a dentist. Parents expressed that the OHCP should be trained to handle special patients (77.9%) and should show empathy (60%). About 48.2% of the parents expressed their concern that their child’s pediatrician never informed them about oral health care, nor referred them to a dentist for consultation. Financial restraints were also a barrier to good oral care.
Conclusion
Accessibility to oral health care facilities with trained OHCPs for special patients was a major challenge faced, and pediatricians should be made aware to refer children to OHCPs at early diagnosis and timely intervention.
Keywords
Access to oral health care
Down syndrome
Oral health
Parents

INTRODUCTION
Down syndrome (DS, also known as Trisomy 21) is a neuro-developmental genetic disorder that is not a disease in itself, but the affected individuals are at a greater risk of acquiring many systemic dysfunctions.[1]
The persons having this syndrome present with intellectual disabilities and an array of medical problems affecting almost all organs, such as heart diseases, impaired visual and hearing acuity, vulnerability to infections, hypotonia, thyroid disorders, and leukemia.[2] DS is reported to be the most common chromosomal abnormality in live-born infants.[3] The United Nations has reported an estimated incidence of DS to be between 1 in 1000 and 1 in 1100 live births worldwide, with approximately 3000-5000 children being born with this chromosome disorder.[4] In India, the numbers are large, and it is reported that over 30,000 children are born with DS annually.[5]
Apart from medical complications, children with DS also present with significant oral and dental health-related challenges and are considered to be at twice the times risk for dental diseases compared to their peers.[6] Anatomical and developmental irregularities in the middle third of the face often result in impaired functions such as chewing, swallowing, and speech. Due to an underdevelopment of the facial middle third, there is a hypoplastic maxilla in relation to the mandible, which, along with a prognathic mandible, results in conditions such as open bite, tongue thrusting, and mouth breathing. Tooth agenesis, hypoplasia, and hypocalcification are often a common clinical finding.[7] Numerous studies have reported poor oral hygiene in such populations, as due to reduced dexterity, these children need assistance in maintaining a proper oral hygiene regime.[8,9] This leads to a high prevalence rate of periodontitis, often manifesting in an aggressive form; however, there have been conflicting reports regarding the incidence of dental caries in such a population. While few authors have reported an increased incidence of dental caries in children with special needs, a systematic review conducted by Martins et al. reported a lower pooled caries incidence compared to the control group.[10,11] But overall, these children have major oral health challenges, which impact their physical and social quality of life.
Parents, who are the primary caregivers for these children, are the ones who have to manage and deal with the day-today challenges of care for these children.[12,13] Various societies and professional bodies have laid down recommendations for screening for cardiovascular status, hearing, and visual acuity shortly after birth, emphasizing regular visits to physicians/pediatricians to monitor these problems.[14] Despite the multiple oro-dental challenges faced by this group of children, dental visits are mostly postponed, neglected, or given a lesser priority than medical examinations.[15] These parents/caregivers often lack guidance and support in terms of providing and monitoring the optimum oral health care of their children.
Although few authors have studied the perception of parents, mothers, or caregivers of children with special needs globally, there is not much published literature in India regarding the same. Thus, the present questionnaire survey was designed with the aim of getting an insight into the parents’ perception regarding the impact of DS on oral health and the challenges faced in availing dental care for their children.
MATERIAL AND METHODS
This study was carried out in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology guidelines. The confidentiality and anonymity of the participant’s information were ensured, and consent was obtained before starting the interview. Initially, semi-structured interviews were conducted in the local language or English language with the parents of children with special needs, and oral health care providers (OHCP) who were enrolled in the panel by purposive sampling. In the second stage, more relevant information was obtained through a literature search pertaining to manuscripts related to oral health needs and challenges of children with special needs. Based on the data obtained, and initial brainstorming sessions, a questionnaire was developed in English Language as it was a pan-India study, and English would be the most understood language. The survey questionnaire was pilot-tested (n = 25) to ensure the practicability, validity, and interpretability of answers and was modified based on the results of the pilot study. For face validity, the questionnaire was distributed among 25 dentists, who rated all the items of the questionnaire on a scale of 1-4, based on the level of clarity and comprehension of the questions (1 = very easy to understand and 4 = very difficult to understand). The questions which were rated 3 and 4 were either modified or removed.
The questionnaire for collecting data was a Google form (https://forms.gle/Ux8wpc7ZYdE7H4Se6). The first section of the form consisted of a declaration explaining the purpose and confidentiality of the survey. The participant’s choice to click the submit button on the first page marked their consent to participate in the study. The respondents were recruited in the study by purposive sampling. The DS Society of India provided the authors with contact details of parents of children having DS. Both convenience sampling (the principal investigator directly contacted the respondents to participate in the study) and snowball sampling (the participating respondents forwarded the questionnaire to their contacts) were used to ensure maximum participation. The survey was shared amongst participants through E-mail and various social media platforms such as Facebook and WhatsApp. The different sections of the questionnaire contain sets of questions about the demographics (nine questions), schooling of the child (three questions), general health of the child (four questions), oral health (seven questions), impact on quality of life, and barriers faced (five questions). The last section was an open-ended question inviting suggestions from the participants [Table 1].
| Demographics |
| 1. Is the respondent mother or father of the child? |
| 2. Mother’s age (in years) |
| 3. Father’s age |
| 4. Mother’s education |
| 5. Father’s education |
| 6. Child’s age |
| 7. Child’s gender |
| 8. The condition child has |
| 9. When did you come to know about the child’s condition? |
| Schooling |
| 10. Does your child attend school? |
| 11. Schooling of the child in a regular or special school |
| 12. Do the teachers in your child’s school train them or you about oral health? |
| General health of the child |
| 13. How do you rate your child’s general health? |
| 14. When was your child’s first pediatrician visit? |
| 15. Did the child’s pediatrician ever inform about oral hygiene or refer you to a dentist? |
| 16. Main problem areas in general health |
| Oral health and hygiene habits |
| 17. Your child’s oral health is |
| 18. Common problem areas in oral health |
| 19. When was the child's first visit to dentist? |
| 20. Did the dentist demonstrate brushing technique? |
| 21. What qualities do you expect in your child's dentist? |
| 22. How does your child clean teeth? |
| 23. What do you do when your child refuses brushing? |
| Impact on child’s quality of life |
| 24. How does child’s oral health impact quality of life? |
| Barriers faced |
| 25. Were you able to find a dentist to cater to a child with special needs? |
| 26. Were you satisfied with services provided by the dentist? |
| 27. What problems have you faced previously with the dentist? |
| 28. Would you appreciate if there is a comprehensive dental program for children with special needs? |
The responses to the Google Form survey were converted into an Excel sheet format for data analysis.
RESULTS
The survey was shared with 225 participants, out of which 201 responded. From these, five forms were excluded because they did not confirm if their children were having DS. Thus, the response rate for the present study was 87% (196/225).
Demographics and educational background
Amongst the respondents, 82.1% were the child’s mother, and 17.9% were the child’s father, mostly in the age range of 35-50 years. About 52% of the mothers and 59% of the fathers were having a postgraduate qualification. Baseline demographics and characteristics of the parents and children are depicted in Table 2. Out of the 195 children, 89.7% had DS, and 9.2% reported Autistic spectrum disorder. One hundred and eleven parents responded that they knew about their child’s condition at the time of the child’s birth or within 6 months of birth. About 78.5% of the parents reported that their children attended school, out of which 47.2% attended regular school, 34.9% attended a special school, and 17.9% were homeschooled.
| Baseline characteristics | Responses |
|---|---|
| Respondent’s relationship with child (%) | Mother 82.9 |
| Father 17.1 | |
| Mother’s education (%) | Highschool 3.1 |
| Intermediate 1.5 | |
| Graduate 43.1 | |
| Postgraduate 52.3 | |
| Father’s education (%) | Highschool 3.6 |
| Intermediate 0.5 | |
| Graduate 39 | |
| Postgraduate 56.9 | |
| Child’s age (in years) (%) | 0-5 (16.9) |
| 5-10 (29.2) | |
| 10-15 (24.6) | |
| 15 plus (29.2) | |
| Child’s gender (%) | Male 53.3 |
| Female 46.7 | |
| Child’s condition (%) | Down’s syndrome 89.7 |
| Cerebral palsy 1 | |
| Autistic spectrum disorder 9.2 | |
| Child’s schooling (%) | Regular 47.2 |
| Special 34.9 | |
| Home-schooling 17.9 |
When asked if the school teaches the children or parents about oral health, only 28.7% responded that schools trained them or children about oral health measures, 44.1% of parents responded that there was no teaching, and 27.2% responded that only sometimes training was there.
General health of the child
Responding to the question, 49.2% of parents responded that it was good, 30.8% said that it was fair, and 17.4% responded that it was very good. They were also asked when their child’s first pediatrician visit was, and 75.9% of parents reported that it was within 1st year of the child’s birth; however, 48.2% reported that the pediatrician never informed them about oral health, neither did they refer the child for a dental consultation.
Among the various general health-related problems in the children, the highest percentage was of speech-related problems (76.9%), followed by problems in vision (36.9%), skin disorders (23.6%), gastrointestinal problems (20%), and heart problems (12.8%).
Oral health and oral hygiene habits of the child
The parents were asked about the status of the oral health of their children, and more than 60% responded that it was good to very good, and 32.3% said that it was not so good. The most common dental problem reported was the presence of cavities (35.4%), open mouth (34.4%), problems in chewing food (29.7%), and teeth grinding (26.7%), followed by malodor, drooling of saliva, thumb sucking, small upper jaw, tongue protrusion, bleeding gums, and collapsed bite [Figure 1].
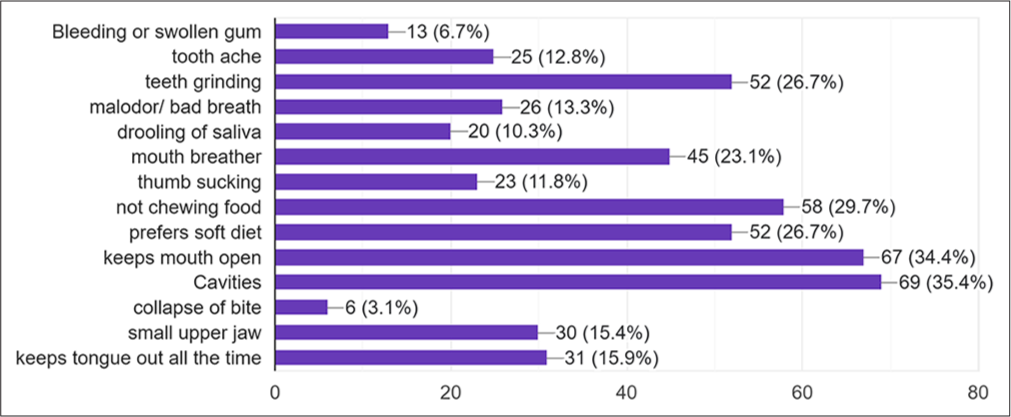
- Graph depicting common oral health issues faced by the children. The numbers outside the bracket represent parent’s response and inside the bracket represent percentage (n=196).
Surprisingly, almost 24% of parents reported that their child has not yet visited a dentist, while only 12.3% had a dental visit within 1 year of the child’s age. The majority of the parents responded that the first dental visit was at the age of 3-6 years (35.4%) and 7-10 years (19%). Among the parents who had visited a dentist, 45.6% reported that the dentist did not demonstrate the brushing technique [Figure 2].
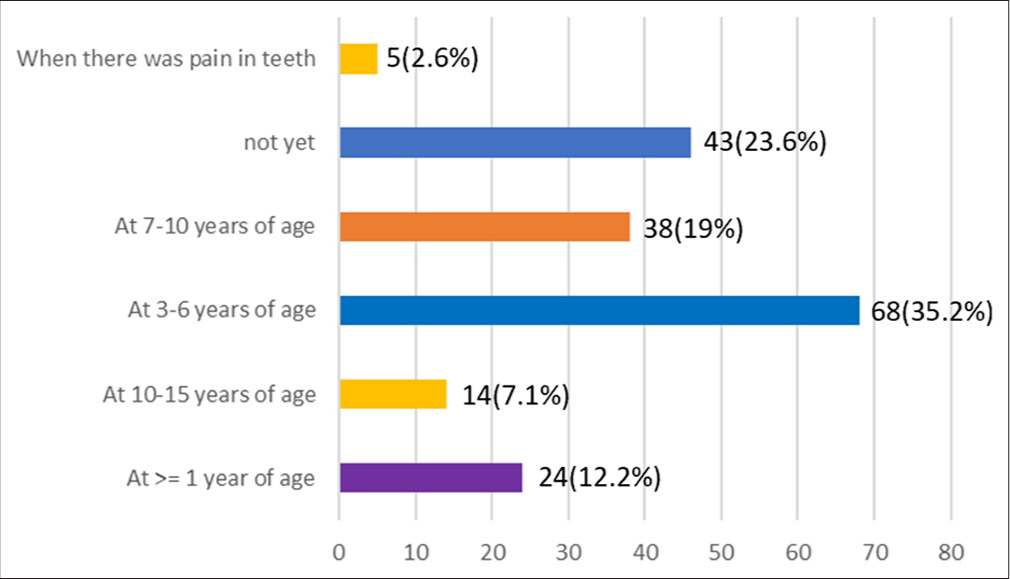
- Graph depicting the responses regarding the age of the child’s first visit to the dentist. The number outside the bracket represents the parent’s response and the number inside the bracket represents percentage (n=196).
Regarding their expectation from the dentist [Table 3], 77.9% of parents responded that they wanted the dentist should know about managing children with special needs, 60% wanted them to be patient and understanding, empathetic (37.9%), should assign extra time for such cases (35.7%), should be a pedodontist (31.8%), should be trained for conscious sedation (26.7%), and should be reassuring (31.3%).
| Desirable quality in a dentist | Response numbers (percentage) |
|---|---|
| Should have knowledge/training to manage special children | 152 (77.9) |
| Should be patient and understanding | 118 (60.5) |
| Should have empathy | 74 (37.9) |
| Should have specially assigned hours for special patients | 70 (35.9) |
| Should be a pedodontist | 62 (31.8) |
| Should be reassuring | 61 (31.3) |
| Should be trained for conscious sedation | 52 (26.7) |
About 49.2% of the parents who responded reported that their child needs assistance from a parent or guardian for tooth brushing, and 49.2% reported that they brushed themselves. About 54.9% of them brushed once a day, 43.1% brushed twice daily, while 2% reported that they brushed after each meal. About 62.6% of parents reported that they adopted an understanding and calm behavior when their child refused to brush their teeth, 36.9% even joined tooth brushing along with the child, 21% reported that they remained firm with the child, 9.2% of parents were forceful, and 3.6% of them did not force the child and left it to that.
Impact on child’s quality of life
When asked about the impact of deranged oral health on quality of life, majority of the parents replied that it largely impacted clarity of speech (65.1%), followed by difficulty in chewing (34.9%), mood swings (25.6%), distress due to toothache (19.5%), social awkwardness (16%), lack of sleep (11.3%), lack of focus (11.3%), and absence from school (8.2%) [Figure 3].
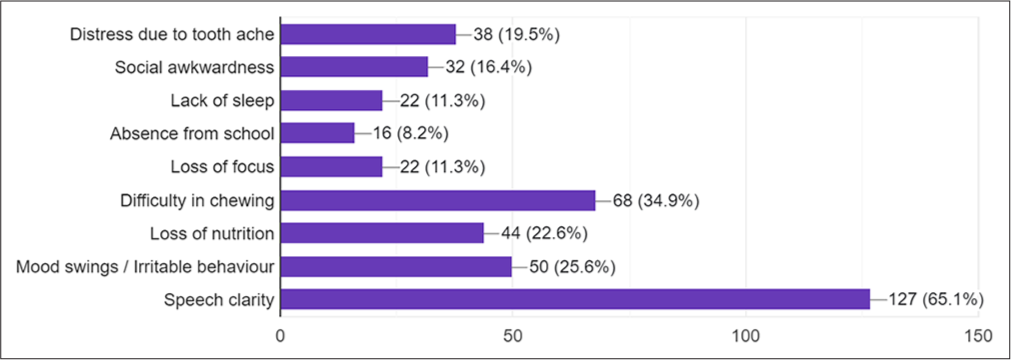
- Graph depicting impact of oral health on quality of life. The numbers outside the bracket represent parent’s response and inside the bracket represent percentage (n=196).
Barriers faced
When asked whether they were able to find a dentist to cater to a child with special needs, only 36.9% answered in an affirmative that they were easily able to find such a dental facility. About 31.3% of parents reported that they are not able to find such a facility yet, 19% reported that they had to travel a long distance to see a dentist, and 12% responded that they could find it, but after much searching and difficulty [Figure 4].
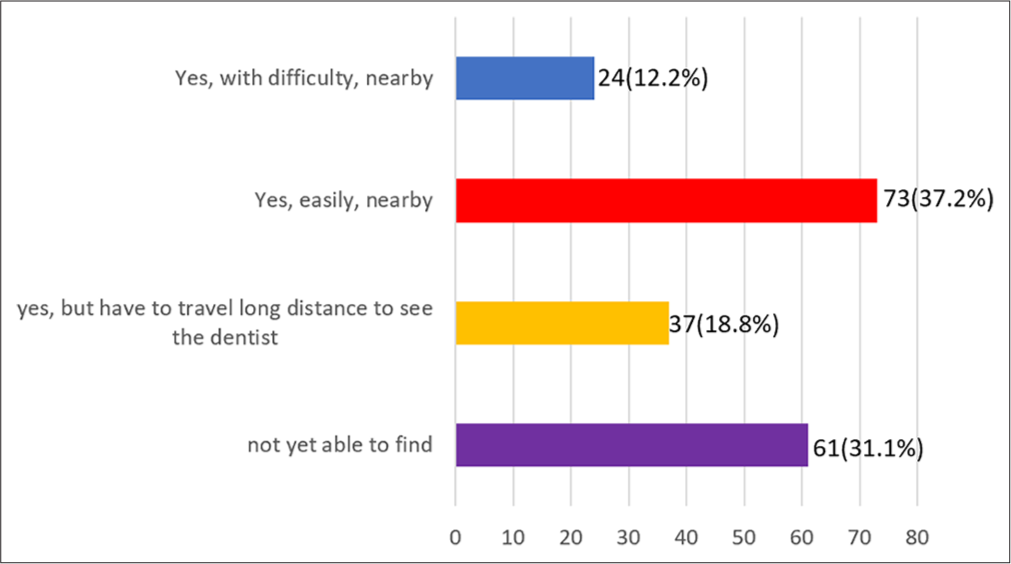
- Graph depicting the difficulty in finding a dentist for special children. The number outside the bracket represents the parent’s response and the number inside the bracket represents percentage (n=196).
While responding to the question of whether they were satisfied with services provided by the dentist, 41.5% responded that yes, they were, 12.8% were not satisfied, while 28.7% said that they would really appreciate it if the dentist was more aware of managing such patients.
Reporting about the problems they faced previously with the dentist, the majority of the parents said that it was difficult to find dentists who could understand the problems of children with special needs and that they lacked sufficient knowledge or skills to handle such patients.
When asked if they would appreciate if there is a comprehensive dental program for children with special needs, 77.4% of parents responded that this is a much-required step as oral care is the most neglected health issue in such patients, and 38.5% of parents also suggested that the pediatricians should be made aware of the importance of dental hygiene [Figure 5].
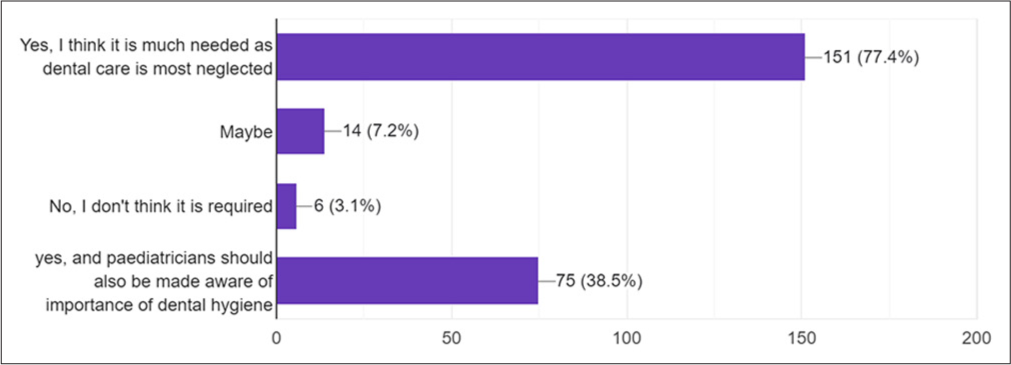
- Graph depicting parents’ desire for a comprehensive dental plan. The numbers outside the bracket represent parent’s response and inside the bracket represent percentage (n=196).
Open-ended section
At the end of the questionnaire, an open-ended section was kept to record the suggestions or opinions of the parents. Most of the parents expressed a need to be trained about oral health measures and techniques they can use for the prevention of oral health diseases in their children. Many reported that the treating dentists are themselves less aware of the management of patients with special needs, so they are not able to guide the parents that well. The parents expect values such as empathy, understanding, and compassion from their dentists while treating their children. Parents even suggested that like a vaccination or pediatrician schedule, there should be a dental visit schedule designed. The schools should be more active in teaching and reinforcing oral health measures in children by organizing workshops, seminars, or lectures for the children as well as their parents.
DISCUSSION
The data and information obtained from the present questionnaire not only depicted what oral health-related problems the children are facing but also the difficulties and barriers faced by their parents to find solutions and treatments for such problems. Previous surveys of parental perceptions regarding the description of the oral health of their children with DS have reported it ranging from overall good oral health[16,17] to others reporting poor.[18]
Access to oral health care and trained OHCPs was a major challenge reported. In the earlier surveys too, this situation has been reported.[19,20] The parents also felt that the OHCPs are themselves not trained or confident enough to handle and manage such patients. One of the parents responded that “management of patients with special needs should be an important and compulsory part of the study for all dental students.” The present dental curriculum does have a few theoretical topics in the syllabus defining special needs conditions, but they are not trained in practical and clinical skills to manage and treat patients with special needs. In a cross-sectional survey study conducted by López et al.[21] among students in Scotland and Brazil, it was found that 83.3% of the dental students who had responded felt that they could benefit from a special care dentistry course or program to manage such patients, and more than 53% of them felt that they did not have adequate knowledge to manage such patients. Similar findings were reported from other surveys conducted in North America,[13] Belgium,[22] and Brazil,[23] where the dentists felt that they needed extra training about patients with DS.
Resounding with earlier surveys and reviews, where high treatment costs were reported as one of the major reasons for not getting dental care,[24-26] here, too, financial aspects were mentioned by the parents. The parents said that they spend a lot of money on therapy and other medical procedures and that they find it difficult to spend much money on the oral health of their children. One of the parents opined in the open-ended section that non-government organizations should help, or government-run hospitals should have trained OHCPs and separate units designated for patients with special needs to provide affordable treatment to such patients.
One of the noticeable findings from the survey was that the child’s first visit to a dentist was not before the age of 3-6 years, and 24% of them had not even had a dental visit yet. There seems to be a definite need to focus on ways that lead to the prevention or reduction of future oral health problems in such children. Early and timely diagnosis is the best method to prevent any disease. Parents need to be educated about the importance of oral health as much as general health, and for this, visits to dentists should be prioritized as much as the pediatrician or physician visit. Pediatricians should also keep oral health considerations in their list and encourage oral health consultation and referrals for children with special needs. In the words of one of the respondents, “A well-defined dental checkup plan and guidelines are the need of the hour, and parents and especially pediatricians should be made aware of them.” Regular visits to the dentists are a must to adopt preventive measures and also for early intervention. In the present study, most of the parents reported that the pediatricians did not advise them about oral health check-ups. The parents also desired that they should be given a set of steps or guidelines for looking after the health of their children, and oral health should be included in the schedule, just like vaccinations and other screenings are included in the schedule.
Almost 50% of the parents reported that their children needed assistance in tooth brushing and maintaining oral health-care regime and that oral health impacts their quality of life in many ways. The main factor affecting life was clarity in speech (65%), followed by difficulty in chewing (34.9%), mood swings (25.6%), toothache (19.5%), and absence from school (8.2%). The oral health difficulties in children with DS affect not only them but also the quality of life of their caregivers and the family as a whole.[27] The responses shown by the parents reflected emotions of loss, sadness, helplessness, and also some kind of anger arising from not being able to help their child well. Thus, catering for oral health is paramount, as it carries a lot of socio-psychological components apart from physical concerns.
The study had certain limitations. As it is a self-reported survey and depends on the honest responses of the participants, it carries the risk of subjectivity bias. Second, definitely, a larger sample size and a more detailed and comprehensive in-depth interview style study design could be planned in the future to get a deeper understanding of the situation and find ways to overcome hurdles to accessing quality oral health care for special patients.
CONCLUSION AND RECOMMENDATIONS
Safeguarding good oral health is much essential for the overall physical, physiological, and psychological health of a person. It is a challenge for oral health providers across the world that patients with special needs, who comprise a large section of society, still have limited access to good oral health care. Not only the patients but their caregivers face the brunt of these challenges. OHCPs and educators, along with medical health care providers and school teachers, need to work synergistically to help and guide the parents and caregivers of children with special needs to provide them accessible, affordable, and quality oral health care. Furthermore, the undergraduate and postgraduate dental curriculum needs to be enhanced so that dental students learn about the cognitive and practical skills to manage patients with special needs.
Ethical approval
The research/study was approved by the Institutional Review Board at Saraswati Dental College and Hospital Lucknow, number #FV1PE25042023, dated April 2023.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
Dr. Vivek Kumar Bains and Dr. Rhythm Bains are part of editorial team, but a blind and impartial review process for the manuscript was ensured.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirms that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Oral health in individuals with down syndrome. Available from: https://www.researchgate.net/publication/221914618_oral_health_in_individuals_with_Down_syndrome [Last accessed on 2024 Jan 20]
- [Google Scholar]
- Oral health considerations for patients with down syndrome. Decis Dent. 2021;7:40-3.
- [Google Scholar]
- Intellectual disability in Western Australia. J Paediatr Child Health. 2000;36:213-5.
- [CrossRef] [PubMed] [Google Scholar]
- Available from: https://www.un.org/en/observances/down-syndrome-day [Last accessed on 2024 Nov 07]
- Down syndrome screening in India: Are we there Yet? J Obstet Gynaecol India. 2017;67:393-9.
- [CrossRef] [PubMed] [Google Scholar]
- Oral disease in children with Down syndrome: Causes and prevention. Community Pract. 2010;83:18-21.
- [Google Scholar]
- Oral health in children with down syndrome: Parents' views on dental care in Flanders (Belgium) Eur J Paediatr Dent. 2015;16:143-8.
- [Google Scholar]
- Dental caries prevalence and treatment needs of down syndrome children in Chennai, India. Indian J Dent Res. 2008;19:224-9.
- [CrossRef] [Google Scholar]
- Oral health condition and treatment needs of a group of Nigerian individuals with down syndrome. Downs Syndr Res Pract. 2007;12:72-6.
- [CrossRef] [PubMed] [Google Scholar]
- Implications of down's syndrome on oral health status in patients: A prevalence-based study. J Family Med Prim Care. 2021;10:4247-52.
- [CrossRef] [PubMed] [Google Scholar]
- The incidence of dental caries in children with down syndrome: A systematic review and meta-analysis. Dent J (Basel). 2022;10:205.
- [CrossRef] [PubMed] [Google Scholar]
- Perception of parents/caregivers on the oral health of children/adolescents with down syndrome. Spec Care Dentist. 2018;38:382-90.
- [CrossRef] [PubMed] [Google Scholar]
- Oral care experiences and challenges for children with down syndrome: Reports from caregivers. Pediatr Dent. 2020;42:430-5.
- [Google Scholar]
- Booklet on practical oral care for people with down syndrome. Available from: https://www.nidcr.nih.gov/sites/default/files/2017-09/practical-oral-care-down-syndrome.pdfm [Last accessed on 2023 Jan 05]
- [Google Scholar]
- Mothers' perceptions concerning oral health of children and adolescents with down syndrome: A qualitative approach. Eur J Paediatr Dent. 2010;11:27-30.
- [Google Scholar]
- Periodontal disease in patients with down syndrome: A systematic review. J Am Dent Assoc. 2018;149:628-39.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of oral health problems in a group of individuals with down syndrome in France. Dev Med Child Neurol. 2000;42:691-8.
- [CrossRef] [PubMed] [Google Scholar]
- Oral health services within community-based organizations for young children with special health care needs. Spec Care Dentist. 2016;36:243-53.
- [CrossRef] [PubMed] [Google Scholar]
- Parental perceptions of unmet dental need and cost barriers to care for developmentally disabled children. Pediatr Dent. 2001;23:321-5.
- [Google Scholar]
- Dental student readiness to treat special care patients upon graduation. Spec Care Dentist. 2023;43:869-82.
- [CrossRef] [PubMed] [Google Scholar]
- Dental care in children with down syndrome: A questionnaire for Belgian dentists. Med Oral Patol Oral Cir Bucal. 2019;24:e385-91.
- [CrossRef] [PubMed] [Google Scholar]
- Dentists' actions about oral health of individuals with down syndrome. Braz J Oral Sci. 2015;14:256-61.
- [CrossRef] [Google Scholar]
- Unmet dental needs and barriers to care for children with significant special health care needs. Pediatr Dent. 2011;33:29-36.
- [Google Scholar]
- Oral health care for patients with developmental disabilities: A survey of Michigan general dentists. Spec Care Dentist. 2018;38:281-90.
- [CrossRef] [PubMed] [Google Scholar]
- Promoting oral health for patients with special needs. Int J Environ Res Public Health. 2023;20:6232.
- [CrossRef] [PubMed] [Google Scholar]




