
Translate this page into:
A novel technique for retrieval of cement-retained crown from an implant abutment and converting it into a combination prostheses

*Corresponding author: Sakshi Sahni, Department of Prosthodontics and Crown & Bridge, Saraswati Dental College and Hospital, Lucknow, Uttar Pradesh, India. sakshisahni2710@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Sahni S, Chopra D, Gaur A, Misra SK. A novel technique for retrieval of cement-retained crown from an implant abutment and converting it into a combination prostheses. Asian J Oral Health Allied Sci. 2024;14:3. doi: 10.25259/AJOHAS_21_2023
Abstract
Dental implant restoration is known to be a widely accepted treatment modality for the replacement of missing teeth and the restoration of masticatory function. Abutment screw loosening is one of the most common causes of failure in single implant-supported restorations, next to loss of osseointegration. Moreover, cement-retained implant-supported prostheses are infamous for their lack of predictable retrievability compared to screw-retained implant-supported prostheses. Management and retrieval of loosening screws are challenging, and this clinical report discusses the procedure for retrieving prosthesis from the abutment of the mandibular molar tooth with minimal damage to the existing restoration, making it possible to be reused.
Keywords
Screw-retained prosthesis
Cement-retained prosthesis
Screw loosening

INTRODUCTION
One of the greatest advancements in the branch of dentistry for the replacement of missing teeth with fixed dental treatment is implants. Implant-supported prostheses can be of two types: Screw-retained and cement-retained. Due to the possibly unpredictable biological and/or mechanical difficulties that may emerge, retrievability of implant-supported dental prostheses is an important aspect of patient treatment.[1] It has been observed that one disadvantage of cement-retained implant-supported prostheses is their lack of predictable retrievability when compared to screw-retained implant-supported prostheses. However, cement-retained prostheses may offer other clinical advantages over screw-retained prostheses, such as greater passivity of fit, lower incidence of ceramic veneer fracture, improved esthetics, lower cost and complexity of laboratory procedures, and the ability to create a more precise occlusion and compensate for malpositioned implants. Predictable retrievable cement-retained implant-supported prostheses would also improve the clinician’s ability to facilitate the maintenance, repair, and replacement of these prostheses as needed.
The purpose of this case report is to describe a technique of retrieval of crown from cement- retained implant abutment and preserving the existing abutment for reuse.
CASE REPORT
A patient aged 29 years reported to the Department of Prosthodontics with a complaint of dislodged restoration for three months. On intraoral examination and radiographic interpretation, implant-supported cement-retained dislodged prosthesis was reported [Figure 1a and b], which has been in function for the past year,with respect to the lower left back region of the jaw. There was inflammation in the buccal mucosa with respect to the same tooth; bone growth was found above; the mesial aspect of the implant collar was confirmed radiographically [Figure 2a]; and the crown prosthesis was attached to the abutment through luting cement. After evaluation, there was no chipping of the veneering porcelain. Therefore, it was decided to reuse the prosthesis. As it was a cement-retained prosthesis, the retrieval of the prosthesis from the abutment was not easy.
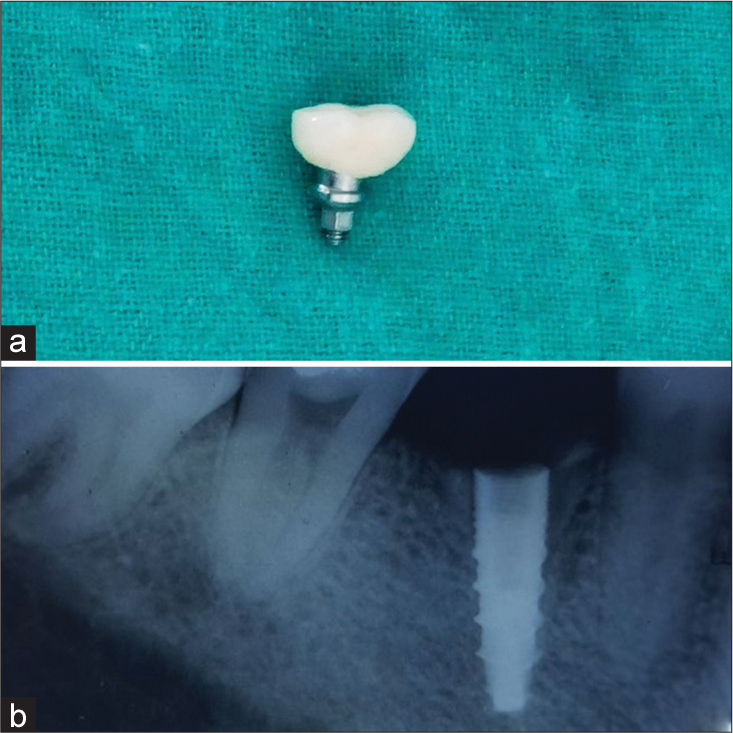
- (a) Dislodged prostheses. (b) Pre-operative radiograph.
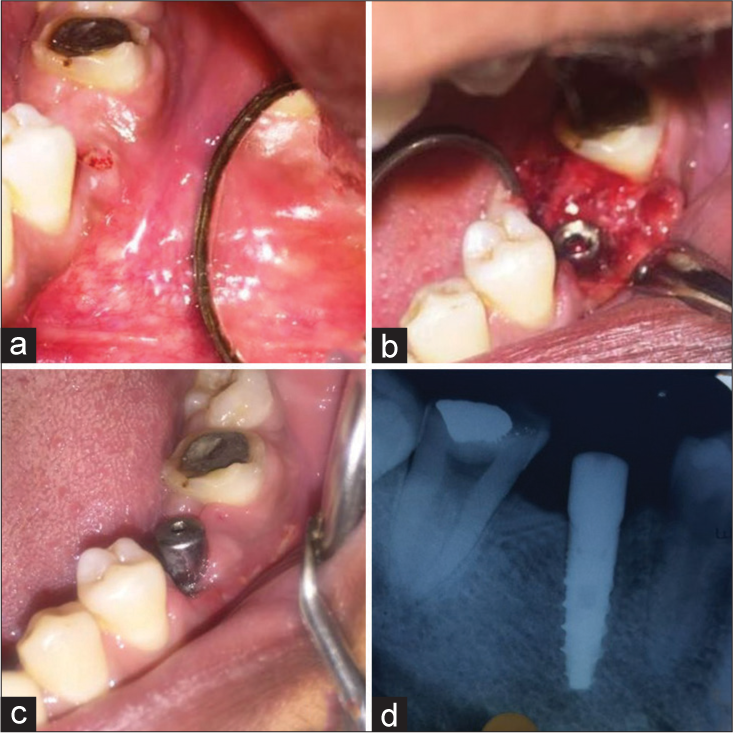
- (a) Bone growth on the mesial aspect. (b) Removal of bone from implant collar. (c) Healing cap and suture removal. (d) Radiographic evaluation.
Technique
To remove the bone from the implant collar, firstly, the mucoperiosteal flap was raised, and the bone was removed with the help of bone cutting bur under local anesthesia [Figure 2b]. A healing cap was placed, and the flap was secured with sutures. The patient was recalled after one week for the suture removal [Figure 2c and d]. The prosthesis was held with an artery forcep, and kept under the ceramic furnace for 10–15 s [Figure 3a]. This caused the cement to soften, and the prosthesis was then detached from the abutment with the help of an explorer [Figure 3b]. Then, cement was removed from the prosthesis and checked for any further retained cement [Figure 3c]. Now, the screw pathway was carefully accessed, and the hole was drilled in the center of the occlusal surface. Once the screw channel was prepared, the fit of the prosthesis to the implant was ensured [Figure 4a]. When the patient arrived at the next appointment, the healing screw was removed. Subsequently, the abutment was torqued to the fixture first, post which the screw access was closed with Teflon tape, and the crown was luted to the abutment. Ensuring the proper occlusion, the screw access was covered with light-cured composite [Figure 4b].

- (a) Prostheses in a ceramic furnace. (b) Detaching crown with explorer. (c) Cement removal.
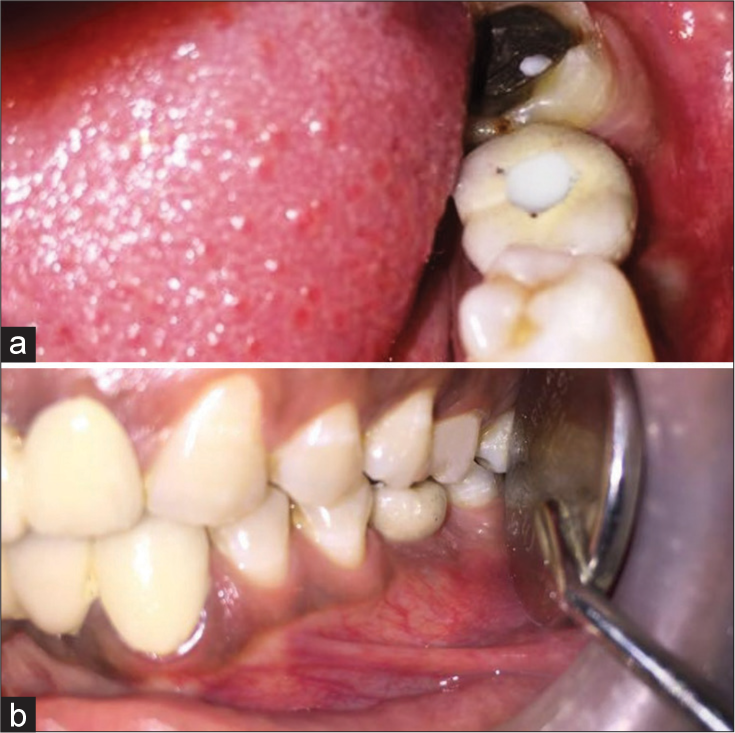
- (a) Fitted prostheses. (b) Prostheses in occlusion.
DISCUSSION
Several clinical studies have reported a higher complication rate for implant-supported restorations in the molar region.[2] The greatest amount of force is generated in the first molar region during mastication, with the chewing occurring mostly in the first molar and second premolar regions. The present report documents the case of screw loosening in a cement-retained prosthesis. A few authors conducted a study related to implants and implant prostheses, and observed that one of the most common peri-implant complications is gingival inflammation or proliferation.[3] As the patient reported to the department with the complaint of dislodged restoration, inflammation was evident in the buccal mucosa with respect to the implant site. This could be due to excess cement around the crown or the complications that occurred at the time of surgery.[4] Pauletto et al. reviewed four cases with cement-retained prostheses, and concluded that any overlaying cement left around the crown of Osseointegrated implants leads to marginal gingival inflammation.[5] This can account for the inflammation with respect to the buccal mucosa. On further inspection, restoration was found attached to the abutment, which had been dislodged from the implant site. Hence, to rectify the mentioned complications, first, a flap was raised to remove the bone from the mesial aspect of the implant site to make the implant collar visible under local anesthesia, and a healing screw was placed. The flap was secured with sutures, and the patient was recalled after one week. The dislodged prosthesis brought in by the patient had no chipped-off veneer, and the anatomy was intact, so a decision was made to reuse it rather than fabricate the new prosthesis. Since prosthesis was attached to the abutment and was cement-retained, its retrieval was difficult. This is one of the most common reasons why many clinicians do not even consider cement-retained prostheses as an option for implant-supported restorations.[6] A technique is performed to detach the prosthesis from the attached abutment order to reuse the prosthesis. The prosthesis with the abutment unit was kept under the ceramic furnace for 10–15 s, which softened the cement, and on exploration with the explorer, it separated from the abutment. The short exposure time in the furnace for the prosthesis was preferred over a complete cycle to preserve the viability of the prosthesis. Too many firing cycles change the shade and weaken the veneer of the prosthesis.[7] This would contribute to the fabrication of a new prosthesis. According to Gober and Weitz, this would also lead the patient to be without the crown for several days and influence the cost as well. Few authors suggest that preparing the access hole in the metal framework of cement-retained prosthesis would increase the survival rate of the prostheses and lowers the cost of maintenance without an increase in porcelain fracture or screw loosening.[8,9] The prosthesis is converted into a screw-retained by drilling a hole in the center of the prosthesis on the occlusal surface,and making an access channel to reach the implant. The cementation of the prosthesis was done with luting cement. With the use of screw-retained prostheses, ease of retrievability is one of the major advantages.[10] Time for the fabrication of a new prosthesis was saved, chair side time was reduced, and the procedure was easy to perform.
CONCLUSION
This clinical report shows the conversion of the existing cement-retained prosthesis into a combination prosthesis. It also reduces the cost of maintenance to the patient without enhancing the risk of porcelain fracture.
Ethical approval
The Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Influence of prosthesis type and retention mechanism on complications with fixed implant-supported prostheses: A systematic review applying multivariate analyses. Int J Oral Maxillofac Implants. 2015;30:110-24.
- [CrossRef] [PubMed] [Google Scholar]
- The effect of implant diameter, restoration design and occlusal table variations on screw loosening of posterior single-tooth implant restotations. J Oral Implant. 2001;27:63-72.
- [CrossRef] [PubMed] [Google Scholar]
- Clinical complications with implants and implant prostheses. J Prosthet Dent. 2003;90:121-32.
- [CrossRef] [PubMed] [Google Scholar]
- Complications associated with excess cement around crowns on Osseo integrated implants: A clinical report. Int J Oral Maxillofac Implants. 1999;14:856-8.
- [Google Scholar]
- Use of lutin agents with an implant system: Part 1. Prosthet Dent. 1992;68:737-41.
- [CrossRef] [PubMed] [Google Scholar]
- Which mechanical and physical testing methods are relevant for predicting the clinical performance of ceramic-based dental prostheses? Clin Oral Implants Res. 2007;3:218-31.
- [CrossRef] [PubMed] [Google Scholar]
- Prosthetic screw loosening: An innovative technique to manage a common complication with dental implants New York: Perio-Implant Advisory; 2016.
- [Google Scholar]
- Reliability of retrievable cemented implant-supported prostheses. J Prosthet Dent. 2016;115:587-91.
- [CrossRef] [PubMed] [Google Scholar]
- A comparison between screw and cement retained implant prostheses? Clin Oral Implants Res. 2007;38:218-31.
- [Google Scholar]




